This issue brief contains corrections.
The United States is home to at least 9 million people who identify as lesbian, gay, bisexual, and transgender, or LGBT. Despite recent advances in social acceptance and legal protections, such as the 2015 U.S. Supreme Court ruling that gave same-sex couples in every state the right to marry, LGBT people and their families across the country continue to face discrimination in areas of everyday life such as employment, housing, and health care.
In order to make meaningful progress in improving the lives of LGBT Americans, policymakers, researchers, advocates, and service providers need more and better data related to the experiences and needs of the LGBT population. Sexual orientation and gender identity, or SOGI, data are a critical component of accurately assessing the current problems that LGBT people experience—such as mental health and substance use disparities and barriers in access to health insurance coverage and health care—and developing effective policies and programs to address them.
Surveys coordinated by the federal government are an essential source of data about the U.S. population. Most major federally supported surveys—including those that assess racial, ethnic, and other disparities that intersect with disparities related to sexual orientation and gender identity—are missing opportunities to collect SOGI data. Fortunately, some surveys are beginning to take steps to gather these data, including the Behavioral Risk Factor Surveillance System, or BRFSS—the largest continuously conducted health survey system in the world.
In 2013, the Centers for Disease Control and Prevention, or CDC, developed a question module for BRFSS to collect data on sexual orientation and gender identity. This SOGI module follows the recommendations of the expert Sexual Minority Assessment and Research Team, or SMART, and the Gender Identity in U.S. Surveillance, or GenIUSS, Group about how to optimally design sexual orientation and gender identity questions. The CDC began giving states the option to add this module to their BRFSS questionnaires in 2014.
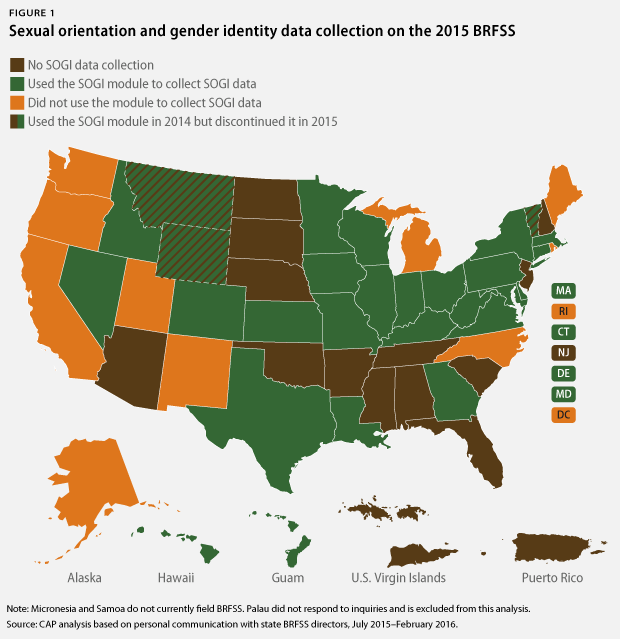
The Center for American Progress analyzed the 2015 BRFSS questionnaires from all 50 states, the District of Columbia, and the U.S. territories currently conducting the survey to determine how many ask about sexual orientation and gender identity and whether they use the SOGI module. This analysis found that 25 states and territories used the module in 2015, up from 20 in 2014. An additional 11 jurisdictions asked about sexual orientation and/or gender identity using questions that differ from the CDC-approved module. In order to most effectively assess and address health disparities affecting the LGBT population, all states and territories should collect SOGI data using the CDC-approved module on their BRFSS questionnaires.
Background on BRFSS
BRFSS, which the CDC coordinates at the U.S. Department of Health and Human Services, or HHS, is an extensive nationwide system of telephone surveys conducted by all states, the District of Columbia, and most U.S. territories. BRFSS annually surveys more than 400,000 American adults about health-related risk behaviors, health conditions, and preventive services and is the premier source of health data that inform a wide range of funding decisions and activities conducted by both public and private actors at the federal, state, and local levels. Many state health departments, for instance, use BRFSS data for purposes such as public education, epidemiology and disease surveillance, policy development, program evaluation, and the compilation of reports on residents’ health. BRFSS data also are cited extensively in scientific journals, including the CDC’s influential Morbidity and Mortality Weekly Report.
The CDC works with state BRFSS coordinators to design the core questions that all BRFSS questionnaires ask. In addition to the required core questions, states and territories may include CDC-approved optional question modules—such as the SOGI module—as well as their own questions. Data gathered via questions designed by individual states and territories are purely for the jurisdiction’s own use. In contrast, the CDC aggregates the data gathered through the required core questions and the optional federally approved modules into a single national pooled data set. The flexible design of BRFSS and its large sample size make it an indispensable tool for the development of national, state, and local research and policy agendas that seek to identify and address health disparities affecting different groups within the U.S. population.
The uses of BRFSS data on sexual orientation and gender identity
Research consistently demonstrates that health disparities are a major concern for the LGBT population. Issues such as discrimination and poverty threaten the health and well-being of LGBT people by increasing risk factors for poor health, such as mental health and substance use; driving a continuing HIV epidemic among transgender women and gay and bisexual men; barring access to appropriate health coverage and care, especially for transgender people; and prompting poor treatment from health care providers who do not understand the needs of LGBT patients. Adding SOGI questions to health surveys such as BRFSS is critical for advocates, researchers, policymakers, and service providers who need comprehensive and accurate data on the LGBT population in order to craft effective responses to these disparities.
CDC-approved SOGI module for BRFSS
The next two questions are about sexual orientation and gender identity.
Do you consider yourself to be:
- Straight
- Lesbian or gay
- Bisexual
- Other
- Don’t know/Not sure
- Refused
Do you consider yourself to be transgender?
- Yes, Transgender, male-to-female
- Yes, Transgender, female-to-male
- Yes, Transgender, gender non-conforming
- No
- Don’t know/not sure
- Refused
INTERVIEWER NOTE: If asked about definition of transgender:
Some people describe themselves as transgender when they experience a different gender identity from their sex at birth. For example, a person born into a male body, but who feels female or lives as a woman would be transgender. Some transgender people change their physical appearance so that it matches their internal gender identity. Some transgender people take hormones and some have surgery. A transgender person may be of any sexual orientation—straight, gay, lesbian, or bisexual.
INTERVIEWER NOTE: If asked about definition of gender non-conforming:
Some people think of themselves as gender non-conforming when they do not identify only as a man or only as a woman.
States that have used this module report that it is well-received by respondents and does not negatively affect the quality of data collected. Missouri State BRFSS Coordinator Janet Wilson noted, for instance, that the state’s experience using the module in 2015 did not result in any survey break-off and had very low rates of item nonresponse.
The experiences of states that already have several years of LGBT population data from their BRFSS illustrate how these data help states create more effective policies and direct limited resources to where they can do the most good.
Massachusetts, for instance, began using state-designed questions on its BRFSS to collect data on sexual orientation in 2001 and gender identity in 2007 before switching to the CDC-approved module in 2015.** These data revealed that LGBT Bay Staters face higher rates of sexual assault, binge drinking, tobacco use, and anxiety and depression than non-LGBT residents. Using these findings, the Massachusetts state government has been able to better target these issues though direct services such as suicide prevention programs, domestic violence prevention and services, homeless services, meals for LGBT elders, and LGBT youth services.
LGBT health disparities in Texas: Exploring a hidden problem
Texas is home to the second-largest LGBT population in the United States: Almost 600,000 Texans identified as LGBT in 2012 and close to 50,000 Texas couples identified themselves on the 2010 census as being in a same-sex relationship. Because of a lack of state-level data collection on sexual orientation or gender identity, very little is known about the well-being of LGBT Texans and their families.
To help address this data gap, the Lesbian Health Initiative of Houston, or LHI, and other partners contacted administrators of a local health needs assessment, the “State of Health in Houston/Harris County,” to highlight national data indicating that almost half of LGBT Texans are uninsured and to underscore how the lack of data related to LGBT health disparities financially burdens the state’s health care system.
Former LHI Executive Director Liz James described LGBT health disparities as “a hidden problem.”
“If you are in the health business in the LGBT world,” said James, “you need to be able to present data so people can understand who we are and how many of us there are. We need them to see us.”
In response, the 2015-16 “State of Health in Houston/Harris County” report cites national data that identify significant LGBT disparities such as homelessness, uninsurance, barriers to health care, and high rates of tobacco use. As part of a commitment to address these issues statewide, the Texas Department of State Health Services added the SOGI module to its BRFSS in 2015.
Colorado asked BRFSS respondents about their sexual orientation with a state-added question from 2006 until the state adopted the CDC-approved SOGI module in 2015. Analysis of the Colorado BRFSS data revealed disparities such as a greater prevalence of smoking, binge drinking, and asthma in the state’s lesbian, gay, and bisexual population compared with the heterosexual population. These data allowed Colorado’s statewide LGBT equality group, One Colorado, to successfully advocate for private funders to invest in an LGBT-specific state health survey in 2012. The findings from this survey, “Invisible: The State of LGBT Health in Colorado,” have guided subsequent policy and programming advances, such as a partnership between One Colorado and the Colorado Department of Public Health and Environment on a transgender-specific statewide health survey based on BRFSS.
These data have also aided in the development of the LGBT Health Outcomes Planning Project as part of the state’s implementation efforts for Healthy People 2020, a partnership with the Colorado Medical Society on a survey of clinicians that revealed a significant need for greater LGBT cultural competency training among the state’s health care workforce, and national investment in efforts by One Colorado and other community partners to address LGBT health disparities in the state’s health insurance marketplace. Numerous other states—including Hawaii, Indiana, North Carolina, and Utah—have similarly used BRFSS data to publish reports on LGBT health.
Collecting BRFSS data on the health of the LGBT population in every state and territory would help local policymakers, service providers, and advocates better address the health disparities and service gaps affecting their LGBT residents. In addition, collecting these data using the standard CDC-approved SOGI module would increase support for these state efforts by allowing for the creation of the most robust nationwide data set ever compiled on the well-being of the U.S. LGBT population.
All states and territories should adopt the SOGI module for their BRFSS questionnaires
In order to obtain a complete picture of the health needs of LGBT individuals in the United States, all states and territories should adopt the CDC-approved SOGI module for their BRFSS questionnaires. The Center for American Progress analysis found that 11 jurisdictions used their own questions to gather sexual orientation and/or gender identity data in 2015. There are three major reasons why these different questions should be replaced with the SOGI module.
The first is that the CDC only incorporates data from the approved SOGI module itself into its national data set. Pooling SOGI data on a national scale is important because while the health disparities affecting this population loom large, the LGBT population itself is estimated to be relatively small: 9 million LGBT people represent about 3.4 percent of the total U.S. population. Some large states, such as California, may be able to gather a sample on their own over one or more years with sufficient statistical power for accurate analyses of disparities affecting the local LGBT population. Pooling these data nationwide, however, allows researchers, policymakers, service providers, and advocates from all states to work with the most statistically robust LGBT population sample possible. The pooled data from the states that used the SOGI module in 2014 are already available for analysis through the CDC website.
Second, consistent wording of questions matters for subsequent analyses. For any concept measured on a survey, even subtle wording changes can result in the collection of data that actually measure different constructs and thus are not directly comparable or able to be easily aggregated.
Finally, the SOGI module represents a best practice in LGBT population statistics because it measures both sexual orientation and gender identity using paired but separate questions. The magnitude of the disparities affecting the transgender population—such as the finding that 41 percent of transgender individuals report having attempted suicide at least once in their lives, a prevalence of lifetime suicidal ideation almost nine times higher than that of the general population—makes it imperative for population surveys to measure gender identity alongside sexual orientation. Measuring gender identity, however, cannot be achieved simply by inserting the option of “transgender” as a response option for a measure asking about sexual orientation. While the disparities affecting groups with a minority sexual orientation—that is, lesbian, gay, and bisexual people—may be very similar to and related to the disparities affecting groups with a minority gender identity—that is, transgender people—sexual orientation and gender identity are different aspects of individual identity and must be measured independently of one another.
Addressing cost barriers to sexual orientation and gender identity data collection in BRFSS
In CAP’s analysis, several states that have not yet added the CDC-approved SOGI module—as well as some of the small number of states that briefly used the module before discontinuing it—cited a lack of funding as the reason for their decisions. Fortunately, the U.S. Department of Health and Human Services has offered to cover the costs of adding the SOGI module at least through 2016.
Even once this funding is no longer available, however, the costs of adding the SOGI module must be weighed against the human and financial costs of allowing discrimination and health disparities to flourish unchecked among the LGBT population. Health disparities incur significant costs to society in the form of poorer overall population health; greater morbidity and mortality from conditions—such as HIV, cancer, and heart disease—that are linked to discrimination, minority stress, and a lack of regular access to health care services; and policies and programs that less effectively target the root causes of poor health among disadvantaged populations.
In order to help states and territories address these issues by adding the SOGI module to their BRFSS questionnaires and retaining it over the long term, HHS should continue financial support beyond 2016 for states that want to use the module. State health foundations and other private funders also should commit to financially support state and territorial health departments in using the SOGI module, and both public and private funders should support special analyses of state-specific and nationally pooled SOGI BRFSS data to help identify LGBT population disparities and formulate appropriate policy and programming responses.
Inclusion of sexual orientation and gender identity questions on other surveys
In addition to BRFSS, other national and state surveys must fully commit to collecting LGBT-specific data. Within the purview of HHS, two priority surveys are the Youth Risk Behavior Surveillance System, or YRBSS, and the National Health Interview Survey, or NHIS.
The YRBSS is the primary source of information on young Americans’ health. The CDC conducts a national YRBSS survey on an annual basis, and states and local jurisdictions annually field their own YRBSS, based on the federal requirements, in a representative sample of schools. Similar to BRFSS, the CDC requires the inclusion of a selected set of questions on the YRBSS questionnaire used by states and local jurisdictions, and states and local jurisdictions are also able to add CDC-approved optional modules and their own questions to their YRBSS questionnaires.
The CDC has approved questions related to sexual behavior and sexual orientation and is working with advocates to develop a measure of gender expression, which is the outward manifestation of an individual’s gender identity through cues such as clothing, hairstyle, and behavior. Over the past several years, numerous local YRBSS surveys have asked these questions, and in 2011, the CDC used these pooled data to publish an analysis of the disparities affecting lesbian, gay, and bisexual, or LGB, youth across the United States. The questions about sexual behavior and sexual orientation began to be included on the national and standard YRBSS high school questionnaires fielded in all states in 2015. To paint a truly complete picture of LGBT youth health, however, the CDC and all states and local jurisdictions administering the YRBSS also should identify issues affecting transgender and gender-nonconforming youth by routinely assessing gender identity and expression.
The NHIS—the federal government’s flagship health survey—is a major source of data on the well-being of U.S. residents. Data from the NHIS are used to track progress toward national Healthy People objectives, provide information for policy decisions on issues such as health insurance coverage, and inform federal and state efforts to reduce health disparities. The NHIS added a question about sexual orientation identity in 2013, and a gender identity measure should be included as well.
In addition to the surveys and other data collection efforts that HHS oversees, other surveys should routinely include demographic questions about both sexual orientation and gender identity. Federally supported surveys that should initiate regular and standardized SOGI data collection include, but are not limited, to:
- American Community Survey (U.S. Department of Commerce)
- Survey of Income and Program Participation (U.S. Department of Commerce)
- Current Population Survey (U.S. Department of Labor)
- National Incident-Based Reporting System (U.S. Department of Justice)
- National Inmate Survey (U.S. Department of Justice)
- National Survey of Veterans (U.S. Department of Veterans Affairs)
Including sexual orientation and gender identity measures as core demographic questions in all these surveys—as well as on state-supported surveys in areas such as employment, criminal justice, and health—would give policymakers, researchers, advocates, and service providers a much-needed thorough understanding of how federal, state, and local agencies can best serve the needs of LGBT people.
Conclusion
Collecting data about sexual orientation and gender identity is vital for meeting the needs of the LGBT population, which is underserved and experiences significant health disparities. It is time for national and state population surveys in the fields of health, employment, criminal justice, military service, and other key policy areas to include questions that allow for a fuller understanding of the experiences of LGBT people and their families. The adoption of the BRFSS SOGI module by 25 states and territories from Guam to Texas to Pennsylvania over just two years—as well as recent federal policy changes such as the Affordable Care Act’s introduction of LGBT-inclusive nondiscrimination protections in health insurance coverage and health care—shows that SOGI data collection is both feasible and timely.*
All states and territories should adopt the BRFSS SOGI module, and other federal and state surveys and agencies should look to this module as inspiration for initiating regular and standardized SOGI data collection in their own surveys and programs. Ultimately, sexual orientation and gender identity measures should be incorporated into all surveys as core demographic questions. Comprehensive data about the extent of disparities affecting the LGBT population in health and other areas allows policymakers, LGBT community advocates, researchers, and service providers to collaborate on effective policy and program agendas that can improve the well-being of LGBT people and their families across the United States.
Kellan Baker is a Senior Fellow with the LGBT Research and Communications Project at the Center for American Progress. Margaret Hughes is a former intern with the Center.
* Correction, March 31, 2016: This sentence has been corrected to accurately reflect that Pennsylvania has adopted the SOGI module, while Florida has not.
** Correction, April 5, 2017: This issue brief incorrectly stated the year in which Massachusetts began collecting BRFSS data on gender identity. The correct year is 2007.